Facial fat grafting for volume restauration with autologous fat grafting
Facial fat descent and atrophy constitute one of the classical aging stigmata (definitely not the most important one, which is ligament relaxation).
This fat is subdivided into anatomically distinct compartments, which can be individually treated. In fact, I have found that strategically injecting fat into these compartments—rather than randomly—greatly enhances the results and gives patients a more natural appearance.
Fat transfer or lipofilling is done by injecting fat from other parts of the body into the face (thighs, abdomen). The fat is injected into specific areas and compartments that are lacking volume, such as the deep medial cheek fat pad, SOOF (cheekbones), Ristow’s space, the chin fat pad, the brow fat pad and the temporal fat pad.
It works extremely well in the undereye area after removing troublesome hyaluronic acid fillers.
This treatment can be performed on its own or in conjunction with other procedures such as facelift, lip lift or brow lift or blepharoplasty surgery.
Transferred fat is more than just a permanent natural filler:
It brings with it adipose-derived stem cells (ADSC), leading to the formation of new blood vessels, collagen and elastin, with a rejuvenated skin.
Cost-effective as one or two sessions can get you the result you need.
Same color hue and feel as normal skin.
Lower risk of infection and allergy compared to fillers.
And here you thought that fat couldn't serve a higher purpose.
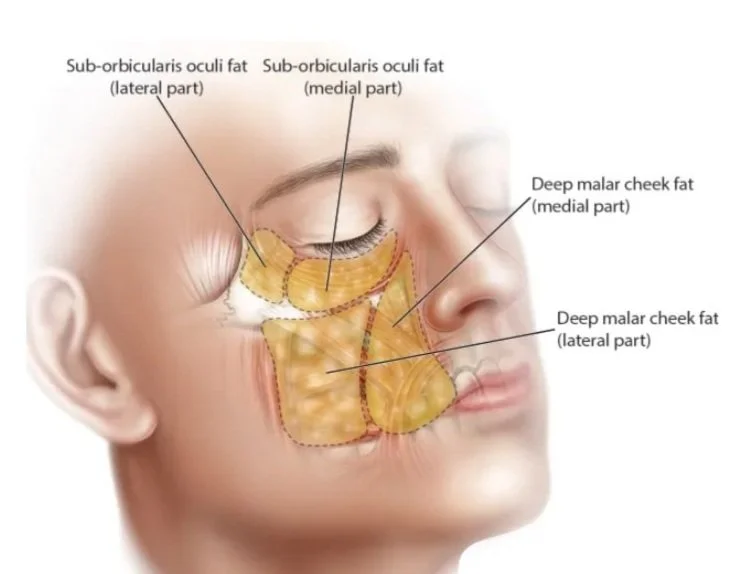
Deep fat pads are mostly the ones who lose volume with time. They should be injected very strategically. (Reproduced from Rohrich, R. Pessa, J. The Fat Compartments of the Face: Anatomy and Clinical Implications for Cosmetic Surgery. Plast. Reconstr. Surg. 119: 2219, 2007.)

Fat grafting done to the deep medial cheek fat pad and SOOF. (Patient at 3 months post-operatively)

Fat grafting to the lower eyelid, tear trough, cheeks, temples and brow fat pads. (Patient at 3 months post-operatively).
Frequently asked questions in my practice
-
Facial fat grafting restores volume lost with aging.
Common areas include the midface, temples, jawline transitions, and periorbital region. The goal is not enlargement, but structural balance, softening shadows and re-establishing continuity between facial units.
Volume should restore proportion. I cannot perform a facelift with fat grafting.
-
Transferred fat that survives becomes living tissue. However, not all injected fat survives (around 70% does).
A percentage of resorption is expected in the early months. Long-term stability depends on technique, recipient site vascularity, and patient-specific factors. Subtle refinement may occasionally be required.
It is not a temporary filler, but it is also not entirely predictable at the millimeter level.
-
It should not.
Overcorrection or poor placement can create heaviness. Conservative layering and anatomical respect are essential. Volume is distributed in planes that restore youthful contours rather than simply adding bulk.
The objective is contour, not fullness.
-
Fat grafting uses your own tissue and is typically performed in a surgical setting. It allows for broader structural contour correction rather than focal volumization.
Fillers are useful for precise, small-volume adjustments. Fat grafting is more appropriate when generalized deflation or multi-area correction is present.
They are tools and not competitors.
Under local anesthesia.
Liposuction on donor site then separation, purification and treatment of the fat.
Reinjection into the deficient area(s) to be treated.
Nanofat (Stem cells and growth factors that come with the fat cells) can be injected or microneedled in the same setting.
No sutures or scars on the face.
Minimal pain with medication.
Minimal swelling and bruising that usually resolve in 1 week.
70-80% of the fat survives (less if you smoke, and less around the eyes and mouth)
Volume does not vary if you keep a stable weight (around 10% of your body weight)
1st Follow-up: 7 days
2nd Follow-up: 3 months to evaluate graft take.
Can usually be combined with a facelift, lip lift, brow lift, or blepharoplasty.
Serving patients in Beirut and Dubai. Dr. Serge Zogheib is a board-certified plastic and reconstructive surgeon practicing in Beirut and Dubai, with a special focus on advanced facial surgery.